XLIF Surgery helps active golfer get back on the course
Dr. Eubanks Helps Patient Put an End to Radiating, Aching Leg Pain
SYMPTOMS & HISTORY
David is a 62-year-old patient who first visited Jason Eubanks, MD, in 2015 due to aching pain in his right leg. A regular golfer, the leg pain resulting from a spine issue was keeping him from the activities he enjoyed. Dr. Eubanks recommended non-operative treatment, and David initially managed the pain with oral anti-inflammatories and physical therapy. Over the next couple of years, Dr. Eubanks also treated him with steroid injections to ease the pain.
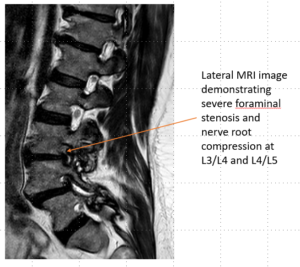
David’s pain persisted despite the non-operative measures he tried. By 2018, his leg pain was rather constant and somewhat debilitating. He was suffering from severe nerve compression, particularly in the neuroforamen (as depicted in the images here), causing his radicular pain in the legs.
DIAGNOSIS
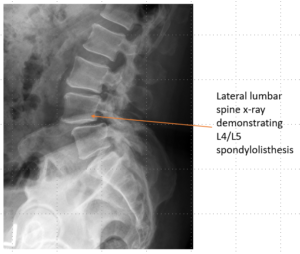
Spondylolisthesis and foraminal stenosis
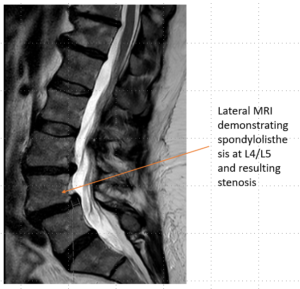
Spondylolysis is the term used for a stress fracture through the pars intra articularis of the lumbar vertebrae. It most commonly occurs at L5/S1 or L4/L5. This stress fracture often does not heal. As a result, as the spine continues to degenerate, the fractured level may slide forward on top of the vertebrae below it. This sliding results in a spondylolisthesis. When it results from a spondylolysis, it is called an isthmic spondylolisthesis.
The most common form of spondylolisthesis, however, results from degenerative arthritic changes in the facet joints of the lumbar spine. This most commonly occurs at L4/L5. The facets remodel and allow the superior vertebrae to slide forward on top of the inferior vertebrae. As a result of this sliding, the lumbar nerve roots can get compressed. This compression (stenosis) often results in leg pain.
TREATMENT
Dr. Eubanks determined that a minimally invasive fusion technique (XLIF) would decompress the nerves and stabilize his spine. See more below for details on this surgery.
Extreme Lateral Interbody Fusion (XLIF)
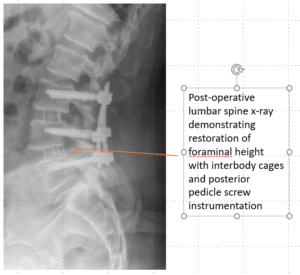
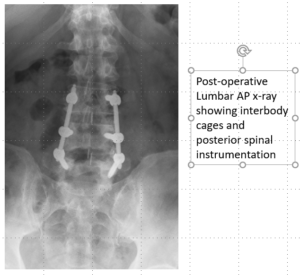
Extreme Lateral Interbody Fusion is a minimally invasive decompression and fusion technique performed through the flank. Special tissue dilators and retractors are used with nerve monitoring to dilate through the psoas (hip flexor) muscle. This allows access to the disc space. Typically, this procedure is performed on the lumbar spine. The disc is taken out, the disc space is distracted to open up the space for the nerves, and a cage with bone graft is then placed in the disc space to keep the nerves decompressed. Often, this lateral fusion technique is supplemented with posterior pedicle screw instrumentation.
This fusion technique is attractive because it has minimal soft tissue disruption and typically very little blood loss. It allows for the restoration of more normal spinal alignment in patients with instability or deformity.
RESULTS
By three weeks after surgery, David no longer had leg pain and was able to go back to the daily activities he enjoyed with no significant restrictions.
WE CAN HELP
If you’re experiencing similar leg pain that you feel may be related to a spine problem, we can help.
Schedule a consultation with Dr. Eubanks at (216) 844-7200.